
Sandeep Mittal
Former Director, LNJN NICFS (MHA)
New Delhi, India
sandeep.mittal@nic.in
Journal of Intellectual Property Rights (JIPR) : [776]
ISSN: 0975-1076 (Online); 0971-7544 (Print)
JIPR Vol.22(6) [November 2017] Page(s): 295-302
|
Abstract: Though the UN has envisaged that accessibility to essential medicines is a basic human right, a large number of people in developing countries are denied access to essential medicines. MNCs having the branded medicines have a tendency to choke the supply chain of cheaper generic medicines using the weapon of intellectual property rights. The TRIPS Agreement has set the minimum standard of protection of Intellectual Property but it has provisions of flexibilities such as compulsory licenses, parallel imports limitations to patent rights, etc., which can be used by member states to provide access to these essential medicines to their people. However, countries like US are using provisions which are over and above the flexibilities incorporated in TRIPS to deny access to essential medicines to people in developing countries. The accessibility of essential medicines to the population in developing countries as affected by these FTAs, ACTA, TPP and TTIP agreements have been examined in this paper and a case has been made out for the unity of the developing and least developed countries to deter US from choking the supply lines of the essential medicines to poor and needy. |
| Keywords: Doha Declaration, TRIPS, Free Trade Agreements, ACTA, TPP, TTIP, intellectual property rights |
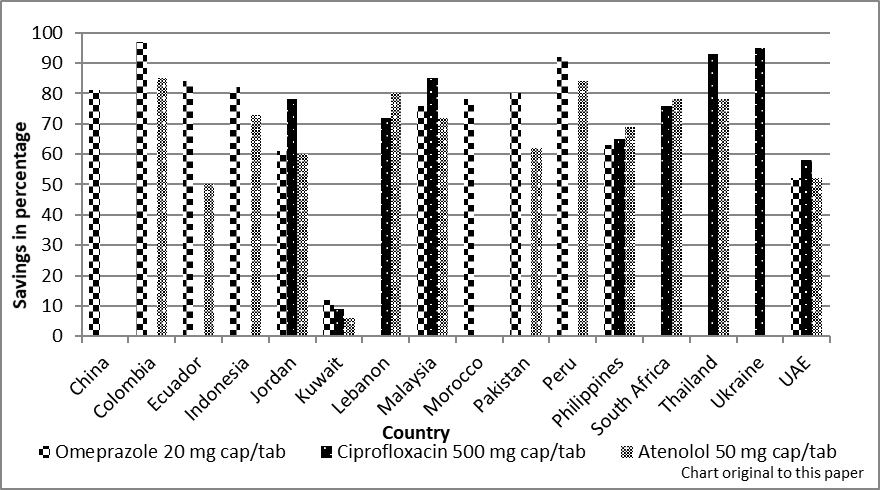
Both the Universal Declaration of Human Rights, 1948, (the Declaration),1 and the International Covenant on Economic, Social and Cultural Rights (the Covenant) require that “medicines are available, accessible, acceptable and of good quality”.2 All the states that are a party to the Covenant have the “legal obligation not to interfere with the rights conferred under the Declaration and the Covenant”.3 However, horizontal and vertical spatial inequalities in healthcare, including in terms of access to medicines, persist throughout the world.4 The mortality rate due to tuberculosis in the WHO African Region during the year 2013 was 42 per a population of 100,000, which is more than twice the global mortality rate (of 16 per a population of 100,000) and 42 times the mortality rate of the WHO American Region (of 1 per a population of 100,000).5 In 2013, in sub-Saharan Africa, out of 25 million people living with HIV, about 64 per cent did not have access to any ART.6 The lack of access to essential medicines in a country is the result of many factors, but the primary reason is the prevalence of high prices of the medicines, stemming from strong intellectual property protection.7 A “secondary analysis of medicine prices, availability, [and] affordability, in 36 developing and middle income countries”8 indicates that the median price difference for originator medicines is substantially higher, reaching up to a whopping figure of 380 per cent as compared to the generic equivalents of these medicines. This reinforces the demand for “switching from originator brand medicines to generic equivalents in the developing countries”, which could facilitate savings of up to 80 per cent on expenditures incurred on essential medicines, as illustrated in Fig. 1.9 Although, the TRIPS Agreement10 lays down minimum standards for the protection of intellectual property, and offers safeguards and flexibilities to prevent patent abuse, the developed countries like the US and the European Union (EU) nations are signing bilateral trade agreements to usurp the flexibilities ingrained in TRIPS. However, the US is consistently and aggressively using such FTAs to deny access to essential medicines to populations in developing countries. Therefore, the scope of this paper is limited to an analysis of the FTAs initiated by US. The flexibilities available in TRIPS are listed out in the paper with the objective of examining how the US is using bilateral FTAs11 and plurilateral (ACTA12, TPP13, TTIP14) agreements to coerce developing countries into accepting stringent ‘TRIPS plus’ provisions for satiating the ever-growing greed of the pharmaceutical industry and denying the poor and needy access to essential medicines. The paper also assesses other factors that constrain the availability of essential medicines for those in desperate need of the latter.
Figure 1 — Average percentage savings obtained by switching from originator brands to lowest priced generic equivalents for three individual medicines in the developing countries15
TRIPS Flexibilities, the Doha Declaration and Public Health
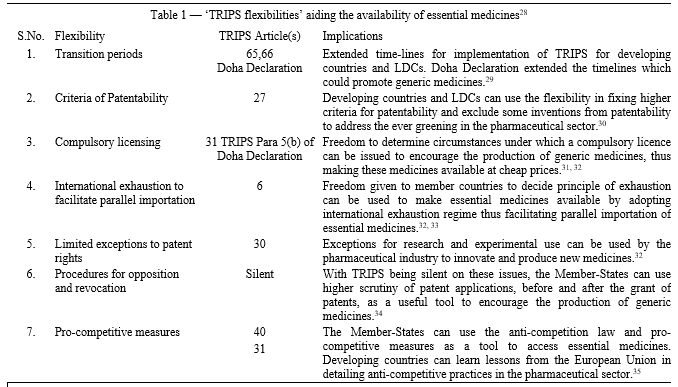
The TRIPS Agreement delineates the minimum global standards for the protection of intellectual property, and offers sufficient liberty (‘flexibilities’) to the Member States to adapt the ‘IP Regimes’ in consonance with their own socio-economic needs. It is legally binding and enforceable through the Dispute Settlement Understanding and is backed by sanctions. A consolidated overview16 of these ‘TRIPS-flexibilities’ aiding the availability of essential medicines is presented in Table 1. The ‘Doha Declaration’17 was adapted after a compromise was reached between the developing countries (mainly India and Brazil) and the developed countries (mainly US), which read as follows:
“We agree that the TRIPS Agreement does not and should not prevent Members from taking measures to protect public health. Accordingly, while reiterating our commitments to the TRIPS Agreement, we affirm that the Agreement can and should be interpreted and implemented in a manner supportive of WTO Members’ right to protect public health and, in particular, to promote access to medicines to all. In this connection, we reaffirm the right of WTO members to use, to the full, the provisions in the TRIPS Agreement, which provide flexibility for this purpose.”18
The Doha Declaration further recognises various flexibilities, “according to and in the light of Paragraph 4 of Declaration, while maintaining commitments in the TRIPS Agreement”.19 Going a step further, it reiterated, and even more explicitly, that public health rights prevail over individual IP rights. This move was possible as the developing countries were well prepared and operated as one block, while also enjoying the active support of international NGOs.7
Recently, UNHRC passed the following resolution,20 despite objections from UK, Switzerland and European Union, which is a big leap for the poor populations in accessing essential medicines,
“1. Recognizes that access to medicines is one of the fundamental elements in achieving progressively the full realization of the right of everyone to the enjoyment of the highest attainable standard of physical and mental health; [OP1, HRC resolution 12/24 and OP 2, HRC resolution 23/14]
2. Stresses the responsibility of States to ensure access for all, without discrimination, to medicines, in particular essential medicines, that are affordable, safe, efficacious and of quality; [based on OP2, HRC resolution 12/24]
3. Calls upon States to promote access to medicines for all, including through the use, to the full, of the provisions of the Agreement on Trade- Related Aspects of Intellectual Property Rights which provide flexibility for that purpose, recognizing that the protection of intellectual property is important for the development of new medicines, as well as the concerns about its effects on prices; [OP7, “g”, HRC resolution 17/14 and OP 5, “h”, HRC resolution 23/14]”
However, in order to benefit from such flexibilities, a country needs to not only frame or amend its national IP laws but also ensure the availability of and access to technology, financial resources, and trained interdisciplinary humanresources. The experiences of developing countries like South Africa,21 Thailand,22, 23 and India24, 25 are indicative of the difficulties being faced by the other developing and the Least Developed Countries (LDCs) in implementing ‘TRIPS flexibilities’ for making essential medicines available to their populations at affordable rates. Significantly, the failure to push through its own public health draft at Doha did not deter the US from using its domestic laws to ‘arm-twist’ countries like Argentina, South Africa and Guatemala by putting them on the ‘USTR 301 Watch List’. This action compelled them to toe the US line in bypassing the “TRIPS flexibilities and accepting ‘TRIPS Plus’ laws to institute more stringent pharmaceutical intellectual property protection”, thereby preventing access to essential medicines in these countries.26 There is no clear definition of ‘TRIPS plus’ but in principle, it refers to commitments that go beyond the TRIPS Agreement.27
The US-FTAs: ‘TRIPS Plus’…or ‘US Plus’…or ‘TRIPS Multiple’…
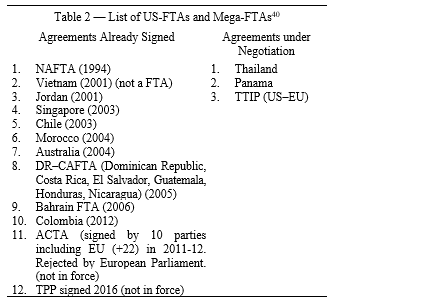
The consistent differential perspective on the standard of protection in TRIPS as the ‘floor’ (minimum standard) of the US and as the ‘ceiling’ (maximum standard) of the developing countries continues to be a driving force behind the aggressive efforts being made by the US to raise the ‘ceiling’, eliminate TRIPS flexibilities and plug loopholes in TRIPS.36 While playing the multi-level, multi-forum global governance card, countries like the US are able to extract TRIPS plus commitments from the economically vulnerable parties through Bilateral Investment Treaties, Bilateral Free Trade Agreements and Regional Free Trade Agreements37 by exerting pressure through the use of the Special 301 clause under the Trade Act, 1974, and the imposition of unilateral sanctions and negotiation of investment treaties.38 The US has signed a slew of such agreements and is currently negotiating a few more as listed in Table 2.
 Most of these stringent provisions, crafted in close nexus with the branded originator drugs pharmaceutical industry,36 aim at promoting originator drugs and eliminating or delaying the entry of generic medicines, thus preventing access to essential medicines at an affordable cost.39 The US–Morocco FTA is considered as the most stringent of all the US FTAs. A summary of the general ‘TRIPS plus’ provisions affecting the availability of essential medicines in the US FTAs is presented in Table 3.
Most of these stringent provisions, crafted in close nexus with the branded originator drugs pharmaceutical industry,36 aim at promoting originator drugs and eliminating or delaying the entry of generic medicines, thus preventing access to essential medicines at an affordable cost.39 The US–Morocco FTA is considered as the most stringent of all the US FTAs. A summary of the general ‘TRIPS plus’ provisions affecting the availability of essential medicines in the US FTAs is presented in Table 3.
*V = Vietnam, J = Jordan, S = Singapore, C = Chile, M = Morocco, A = Australia, D = DR-CAFTA, B = Bahrain

Consider the views of the pharmaceutical industry on TRIPS plus provisions, as put forward by Micky Kantor,44 a former USTR turned lobbyist for the pharmaceutical industry, while trying to explain that the provisions of free trade agreements are not violative of the TRIPS Agreement, which reads as follows:
“Characterizing these provisions as TRIPS-plus is misleading,…. While it is true that these provisions often are more specific and provide greater intellectual property protection than that provided by the TRIPS Agreement, that does not mean they violate the TRIPS Agreement.”45
However, subsequently in the same document, he made his dubious intention clear, which read:
“Article 31, the Doha Declaration and the Paragraph 6 Compromise are fundamentally ‘exceptions’ to the intellectual property protections embodied in the TRIPS Agreement…..But these exceptions can not swallow the rule: strong intellectual property protections remain essential to foster innovation and creativity.”46
An analysis of the TRIPS plus provisions listed above leaves no doubt that these FTAs undermine the TRIPS flexibilities with their intention to block the supplychain of generic medicines and are thus fatal in terms of ensuring accessibility to essential drugs.31, 47
The Free Trade Agreements, from Bilateral to Plurilateral Mechanisms
The success in coercing many countries to sign FTAs encouraged the US to take bilateral negotiations to the next higher level of plurilateral negotiations. The US had been unsuccessful in imposing its own intellectual property standards on the developing countries since the advent of the TRIPS and Doha negotiations. Consequently, it began negotiating bilateral trade agreements, with each successive agreement building more ‘pluses’ on the predecessors, to achieve a cumulative effect,49 and creating more regional trade blocks likes ACTA, TPP and TTIP. The negotiations for these regional agreements were shrouded in secrecy, away from the gaze of the public and NGOs, to avoid pre-emption of their next moves by these democratic stakeholders. When some of these draft agreements were leaked into the public domain, there was a hue and cry because of their ominous implications for civil liberties and access to essential medicines. The European Parliament rejected it, despite the fact that the EU and its 22 members had signed the agreement. The TPP has been signed in 2016, but is still not in force while the TTIP is still under negotiation. The TPP and TTIP together would be the largest critical mass of support for ‘US-forced’ TRIPS plus laws (Fig. 2).
When the Senate passed the Trade Promotion Authority, the US President termed itas “……an important step toward ensuring [that] the United States can negotiate and enforce strong, high- standards trade agreements…..”.49
A summary of the TRIPS plus provisions in the ACTA and TPP and their effects on the availability of affordable medicines is presented in Table 4, clearly pointing to a systematic attempt to create more stringent standards, thus increasing the “barriers to access generic medicines either by intensifying such IP protections as existence and duration of exclusivity or by reducing the use of flexibilities such as compulsory licenses or parallel import”.50 The introduction of third-party liabilities, exemplary deterrent penalties and criminal offences illustrates how the US is determined to choke the global supply lines of essential medicines.
Figure 2: Schematic map showing the emergence of a Mega Free Trade Area


The US Government explicitly leveraged bilateral FTAs to influence regional and multilateral negotiations on ‘TRIPS plus’, thus triggering the onset of plurilateralism through six distinct mechanisms, viz., “chain reaction, pressure for inclusion, coalition building, emulation, legal interpretation and adherence”. This has fostered instability and fragmentation among the WTO members.55 The ‘TRIPS plus’ bilteral, regional and plurilateral agreements have also made it difficult for the affected populations to access essential medicines not only due to the lack of capacity and resources but more so because of strikes by the developed countries. This prompted the developing countries to strike back at the WTO, WIPO, and international regimes, giving rise to fears of a potential TRIPS-war.56, 57 If a sufficient number of countries sign these agreements, leading to the adoption of TRIPS plus standards, theUS would be able to use Article 4 of TRIPS to legitimately exert pressure upon multilateral forums like the WTO and WIPO,50 for laying down new international standards in line with the TRIPS plus provisions.48 The intellectual property protection regime is hence seen to be monopolistically shifting from the ‘TRIPS plus’ to a ‘TRIPS multiple’ regime in congruence with the US Government’s ‘military– political’ goals.58
However, access to essential medicines is also dependent on the political will and policies of individual countries. Public interest groups and NGOs play a crucial role in improving accessibility to medicines. Ensuring stringent checks on corrupt practices by pharmaceutical companies and procurement officials would also help improve the situation. The capacity building of countries in terms of technology and human resources for generic manufacturing would be an important factor in making countries self-reliant in the manufacture of generic medicines. However, the apprehension persists that geo-political considerations may influence governments to succumb to pressures from their military allies, compelling them to fall in line with the efforts of the US to block access to generic medicines throughout the world.
Conclusion
The right to public health, including access to essential medicines, is a basic human right and has precedence over the individual right of intellectual property. Ample flexibilities in this regard have been incorporated in the TRIPS Agreement and have been reiterated in the Doha Declaration. However, countries like the US are using the mechanism of bilateral and plurilateral FTAs having ‘TRIPS plus’ provisions to usurp these ‘TRIPS flexibilities’ for denying access to essential medicines to populations in developing and least developed countries. The emerging mega-regionals like ACTA, TPP and TTIP would worsen the situation by putting the affected populations to more hardships. The developing and least developed countries need to unite to prevent the US from altering the international law in world trade in the near future. In addition, international NGOs, all citizens, legislators and the judiciary in these countries need to become decisively proactive to ensure the uninterrupted supply of essential medicines for the public. This can be achieved only by curtailing the hegemony of the West and allowing the less developed nations to exercise their prudence and freedom to make essential medicines easily available for their populations while keeping the complicated issue of patents at bay.
VII. REFERENCES
- 1 Universal Declaration of Human Rights, ed. United Nations (United Nations, 1948), Article 30.
- 2 International Covenant on Economic, Social and Cultural Rights, in Treaty Series, 993, p.3, ed. United Nations (UN General Assembly, 1966), Article 12.
- 3 International Covenant on Economic, Social and Cultural Rights, in Treaty Series, 993, p.3, ed. United Nations (UN General Assembly, 1966), Article 5.
- 4 The World Health Report 2008: Primary Health Care Now More Than Ever, World Health Organization, 2008.
- 5 World Health Statistics 2015, in Geneva: WHO, ed. World Health Organization (Geneva: World Health Organization, 2015), fig. 7,3rd graph.
- 6 World Health Statistics 2015, in Geneva: WHO, ed. World Health Organization (Geneva: World Health Organization, 2015), fig. 5.
- 7 Ellen FM’tHoen, TRIPS, pharmaceutical patents and access to essential medicines: A long way from Seattle to Doha, Chicago Journal of International Law, 3 (1) 2002.
- 8 Alexandra Cameron et al., Medicine prices, availability, and affordability in 36 developing and middle-income countries: A secondary analysis, The Lancet, 373 (9659) 2009.
- 9 Alexandra Cameron et al., Switching from originator brand medicines to generic equivalents in selected developing countries: How much could be saved?, Value in Health, 15 (5) 2012.
- 10 Agreement on Trade-Related Aspects of Intellectual Property Rights, ed. World Trade Organization, 1869 UNTS 299; 33 ILM 1197 (1994), World Trade Organization, 1994.
- 11 Free Trade Agreements signed by US with several countries under Trade Promotion Authority Act, 2002, which mandates IP protection in bilateral and multilateral agreements similar to US Domestic Law.
- 12 Anti- Counterfeiting Trade Agreement, 2010, 10 of the 11 negotiating parties [Australia, Canada, EU (+22 members), Japan, Mexico, Morocco, New Zealand, Singapore, South Korea, Switzerland, United States] signed by 2012, except Switzerland. The 22 EU Member countries also signed. So far only Japan has ratified. European Parliament rejected ACTA on 4 July 2012 on grounds of potential threat to civil liberties.
- 13 Trans-Pacific Partnership Agreement, 2016 (signed but not in force). An attempt by US to unite 12 countries in Pacific Rim.
- 14 Transatlantic Trade and Investment Partnership, ed. US and EU (Under Negotiation).
- 15 Cameron et al., Switching from Originator Brand Medicines to Generic Equivalents in Selected Developing Countries: How Much Could Be Saved?, Table 5, Value in Health, 15(5) (2012) 664 -73.The Graph in this paper is drawn by using this secondary data.
- 16 Cameron et al., Switching from Originator Brand Medicines to Generic Equivalents in Selected Developing Countries: How Much Could Be Saved?, Table 5, Value in Health, 15(5) (2012) 664 -73. Consolidated Table is original to this paper.
- 17 Declaration on the TRIPS Agreement and Public Health adopted on 14 November 2001, Doha WTO Ministerial 2001: TRIPS, ed. DOHA WTO MINISTERIAL 2001: TRIPS, WT/MIN(01)/DEC/2, and 20 November 2001 (Doha 2001).
- 18 Declaration on the TRIPS Agreement and Public Health adopted on 14 November 2001, Doha WTO Ministerial 2001: TRIPS, ed. DOHA WTO MINISTERIAL 2001: TRIPS, WT/MIN(01)/DEC/2, and 20 November 2001 (Doha 2001), para 4.
- 19 Declaration on the TRIPS Agreement and Public Health adopted on 14 November 2001, Doha WTO Ministerial
2001: TRIPS, ed. DOHA WTO MINISTERIAL 2001: TRIPS, WT/MIN(01)/DEC/2, and 20 November 2001 (Doha 2001), para 5. - 20 UNHRC, Draft Resolution on Access to medicines in the context of the right of everyone to the enjoyment of the highest attainable standard of physical and mental health,32nd Session, Agenda No. 3 (2016).
- 21 Patrick B, Globalization, Pharmaceutical pricing, and South African health policy: Managing confrontation with US firms and politicians, International Journal of Health Services, 29 (4) 1999.
- 22 Mohara A et al., Impact of the introduction of Government use licenses on the drug expenditure on seven medicines in Thailand, Value in Health, 15 (1) 2012.
- 23 Akaleephan C et al., Extension of market exclusivity and its impact on the accessibility to essential medicines, and drug expense in Thailand: Analysis of the effect of TRIPS-Plus proposal, Health Policy, 91 (2) 2009.
- 24 Kapczynski A, Harmonization and its discontents: A case study of TRIPS implementation in India’s pharmaceutical sector, California Law Review, 97 (6) 2009.
- 25 Lee Linda L, Trials and TRIPS-ulations: Indian Patent Law and Novartis Ag v Union of India, Berkeley Technology Law Journal, 23 (1) 2008.
- 26 Ghanotakis E, How the US interpretation of flexibilities inherent in TRIPS affects access to medicines for developing countries, The Journal of World Intellectual Property, 7 (4) 2004.
- 27 David Vivas-Eugui, Regional and Bilateral Agreements and a TRIPS-Plus World: The Free Trade Area of the Americas (FTAA), Quaker United Nations Office (QUNO), 2003.
- 28 Grover A, Report of the Special Rapporteur on the Right of Everyone to the Enjoyment of the Highest Attainable Standard of Physical and Mental Health, UN General Assembly, Human Rights Council, 2009.
- 29 Deere C, The implementation game: The TRIPS Agreement and the global politics of intellectual property reform in developing countries, OUP Oxford, 2008.
- 30 Indian Patents Act, 1970, Section 3(d).
- 31 Abbott Frederick M & Reichman Jerome H, The Doha Round’s public health legacy: Strategies for the production and diffusion of patented medicines under the amended TRIPS provisions, Journal of International Economic Law, 10 (4) 2007.
- 32 Cecilia Oh, Compulsory licences: Recent experiences in developing countries, International Journal of Intellectual Property Management, 1 (1-2) 2006.
- 33 Musungu Sisule F & Cecilia Oh, The Use of Flexibilities in TRIPS by Developing Countries: Can They Promote Access to Medicines? World Health Organization, South Centre Geneva, 2006.
- 34 Nathan Ford et al., The role of civil society in protecting public health over commercial interests: Lessons from Thailand, The Lancet, 363 (9408) 2004.
- 35 Developing countries can take lesson from European Union in detailing anti-competitive practices in pharmaceutical sector, Domanico Fabio & Kamilarova Elena, Final results of the commission pharmaceutical sector inquiry: Competition and regulatory concerns to address, Antitrust, 2009.
- 36 Susan K Sell, TRIPS-Plus free trade agreements and access to medicines, Liverpool Law Review, 28 (1) 2007.
- 37 Abbott Frederick M, Intellectual property provisions of bilateral and regional trade agreements in light of US Federal Law, UNCTAD-ICTSD Project on IPRs and Sustainable Development, Issue Paper, no. 12, 2006.
- 38 Jorge María Fabiana, TRIPS-Plus provisions in trade agreements and their potential adverse effects on public health, Journal of Generic Medicines: The Business Journal for the Generic Medicines Sector, 1 (3) 2004.
- 39 Correa Carlos María, Implications of bilateral free trade agreements on access to medicines, Bulletin of the World Health Organization, 84 (5) 2006.
- 40 Fink C & Reichenmiller P, Tightening TRIPS: Intellectual property provisions of US Free Trade Agreements, Trade, The World Bank Group Trade Note, 7 February 2005.
- 41 Fink C, Entering the jungle of intellectual property rights exhaustion and parallel importation, Intellectual Property and Development: Lessons from Recent Economic Research, Oxford, UK: Oxford University Press/Washington, DC: World Bank, 2005.
- 42 Krikorian Gaëlle P & Szymkowiak Dorota M, Intellectual property rights in the making: The evolution of intellectual property provisions in US Free Trade Agreements and access to medicine, The Journal of World Intellectual Property, 10 (5) (2007).
- 43 Jorge M F, TRIPS-plus provisionsin trade agreements and their potential adverse effects on public health, Journal of Generic Medicines, 1 (2004) 199–211.
- 44 Kantor M, US Free Trade Agreements and the Public Health, Submission to the WHO’s Commission on Intellectual Property Rights, Innovation, and Public Health, http://www.who.int/intellectualproperty/submissions/US%20FTAs%20a nd%20the%20Public%20Health.pdf, 2005.
- 45 Kantor M, US Free Trade Agreements and the Public Health, Submission to the WHO’s Commission on Intellectual Property Rights, Innovation, and Public Health, http://www.who.int/intellectualproperty/submissions/US%20FTAs%20a nd%20the%20Public%20Health.pdf, 2005, p. 3.
- 46 Kantor M, US Free Trade Agreements and the Public Health, Submission to the WHO’s Commission on Intellectual Property Rights, Innovation, and Public Health, http://www. who.int/intellectualproperty/submissions/US%20FTAs%20a nd%20the%20Public%20Health.pdf, 2005, p. 9.
- 47 Fink C, Entering the jungle of intellectual property rights exhaustion and parallel importation, Intellectual Property and Development: Lessons from Recent Economic Research, Oxford, UK: Oxford University Press/Washington, DC: World Bank, 2005; Fink C & Reichenmiller P, Tightening TRIPS: Intellectual property provisions of US Free Trade Agreements, Trade, The World Bank Group Trade Note, 7 February 2005.
- 48 Drahos P, Bits and Bips, The Journal of World Intellectual Property, 4 (6) 2001.
- 49 Statement by the President on Senate Passage of Trade Promotion Authority and Trade Adjustment Assistance, News Release, 2015, https://www.whitehouse.gov/the-press-office/2015/05/22/statement-president-senate-passage-trade-promotion-authority-and-trade-a.
- 50 Krikorian G P & Szymkowiak D M, Intellectual property rights in the making: The evolution of intellectual property provisions in US Free Trade Agreements and access to medicine, Journal of World Intellectual Property, 10 (5) (2007) 388–418, at 393.
- 51 Flynn Sean M & Madhani B, Acta and access to medicines, The Greens, European Free Alliance, 2011.
- 52 Weatherall K, Politics, compromise, text and the failures of the Anti-Counterfeiting Trade Agreement, Sydney Law Review, 33, 2011.
- 53 Baker B K, Acta-Risks of third-party enforcement for access to medicines, American University International Law Review, 26 2010.
- 54 Jaeger T, Merging Acta into TRIPS: Does TRIPS-Based IP Enforcement Need Reform?, in TRIPS Plus 20, From Trade Rules to Market Principles, ed. Hens Ulrich, Reto M, Hilty, Matthaias Lamping & Joseph Drexl, Heidelberg: Springer, 2016.
- 55 Morin Jean‐Frédéric, Multilateralizing Trips‐Plus Agreements: Is the US strategy a failure?, The Journal of World Intellectual Property, 12 (3) 2009.
- 56 Peter K Yu, The rise and decline of the intellectual property powers, Campbell Law Review, 34 2012.
- 57 TRIPS Wars: Developing Countries Strike Back, 2016, http://goo.gl/irhKcQ.
- 58 Pérez-Rocha, The Transatlantic Trade and Investment Partnership (TTIP): Why Should the World Beware, Brussels, Rosa-Luxemburg-Stiftung, 2015.

0 comments on “Effects of TRIPS Plus Provisions in International Trade Agreements upon Access to Medicines in Developing Countries”